
One and a half million dollars. This is how much money—annually— my hometown hospital in rural Kentucky has lost since 2012. With less than a week’s worth of operating cash on hand at any given time, the small rural hospital has been struggling to make ends meet for years now. This is not the only rural hospital in Kentucky with this problem; there have been five rural hospital closures in the state since 2009, four of them shutting down since 2014. And according to a study conducted by Navigant in 2019, there are another sixteen rural hospitals in Kentucky at high risk of shutdown, and thirty-five more in poor financial health. However, it wasn’t until the last decade that rural hospital closures in the state have increased at such a rapid rate. Why is this?
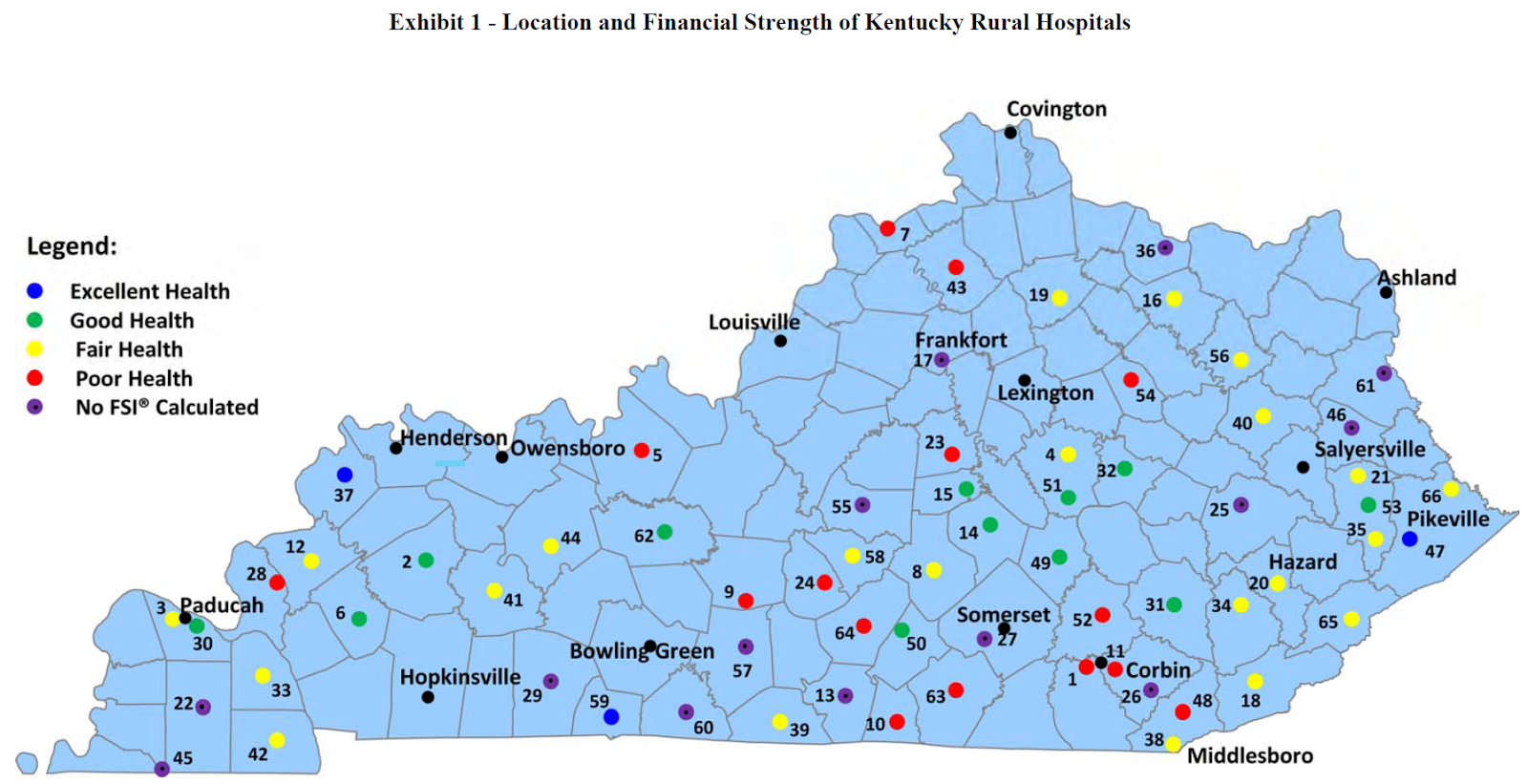
Source: Kentucky Health News
Rural Hospital Closures: At the Surface
In order to get to the root of the problem for rural hospitals, it is important to first examine its various layers. At the surface, many of the financial constraints rural hospitals face are largely due to the way Medicare (which provides coverage to roughly 900,000 Kentuckians) reimburses hospitals for the services provided.
To put it into context, when a patient on Medicare is treated, Medicare reimburses the hospital a flat fee depending on a patient’s diagnosis, or Diagnosis Related Group (DRG). This payment is the product of two components: (1) a standardized amount for the diagnosis, which is adjusted depending on the average wage level in the area that the hospital is located, and (2) the DRG’s relative weight, or severity of the diagnosis. This payment system is known as the Inpatient Prospective Payment System (IPPS). The DRG assigned can be influenced by the patient’s age and gender, and multiple DRGs can be assigned to a patient during a single stay. Thus, regardless of what a hospital may normally charge for a particular service provided to a private insurance patient, they must agree to charge Medicare patients a set price for that same service.
So why has this reimbursement system failed rural hospitals in Kentucky as much as it has? There are a number of contributing factors. One of the primary reasons is that under a reimbursement model like Medicare where the average wage level of an area is a determinant in how much is paid back to the hospital, states like Kentucky are put at a disadvantage. This is due to the fact that the majority of Kentuckians live and work in rural, lower-than-average wage level parts of the state, and thus, hospitals here have historically been paid less under the Medicare program than hospitals in urban/higher wage level areas. For instance, a hospital in a low-wage, rural community could receive a Medicare payment of about $4,000 for treating a beneficiary admitted for pneumonia. However, a hospital in a high-wage, urban area could receive a Medicare payment of roughly $6,000 for the same diagnosis due to wage index differences. Not only does this leave a growing shortfall of uncompensated care costs for a rural hospital, but it also perpetuates its inability to provide high-quality care because its low wage levels disincentivize skilled physicians to work there. Many rural hospitals have tried to hire a larger variety of doctors—and not just those that practice primary care—in order to attract more private insurance patients, however, this has been a difficult task considering there is a near 10 percent difference in salary for physicians working in urban areas versus rural areas.
And in turn, the lack of skilled hospital personnel has largely affected a rural hospital’s efficiency, and thus, how much money it makes. For example, if a Medicare patient gets treated at a hospital, Medicare essentially gives the hospital x amount of money for the number of days it should take to treat a patient with a certain diagnosis. If the hospital can discharge the patient sooner than that amount of days, they still get x amount of money, and if it takes them longer than the required amount of days to discharge the patient, they are still going to get x amount of money. Therefore, if a hospital is in an urban or higher wage level area and has a variety of skilled physicians that can provide a number of services, they can oftentimes discharge a patient sooner than the number of days they were paid for, and therefore make somewhat of a profit. On the other hand, if a hospital is in a rural area with fewer resources and physicians, they often struggle to discharge the patient in the number of days they were reimbursed for, and thus, end up losing money.
More than half of Kentucky’s rural hospitals operate under this kind of reimbursement model. However, 28 of Kentucky’s 65 rural hospitals are classified as Critical Access. These are hospitals that operate with less than 25 acute care beds and are at least 35 miles from another acute care facility. Under this designation, diagnosis and wage level are not factored into how much money is reimbursed when treating a Medicare patient, and hospitals are simply reimbursed for the services provided. Though this reimbursement model has good intentions, it still fails to sufficiently finance rural hospitals because it does not cover the hospital’s other operating costs, like gas, water, purchasing new equipment, or keeping the light’s on over the patient’s head. Rural hospitals must use the little profit they make off of private insurance patients to cover these costs, and when nearly 75-80 percent of the patients rural hospitals treat are on Medicare or Medicaid, this does not leave a Critical Access Hospital a lot of money to work with.
Regardless of their designation, though, all hospitals were subject to cuts in the Medicare program under the Budget Control Act of 2013, which has largely contributed to the financial distress of many rural hospitals. In hopes to mitigate federal spending by $1.2 trillion over a period of nine years, Congress reduced Medicare reimbursement payments to hospitals by 2 percent. Though this meant that there weren’t any changes in the patient’s copay or deductible amount, Medicare was now required to reimburse hospitals 98 cents per dollar of their share, leaving the hospital to cover the uncompensated costs. And in rural hospitals like that of my hometown where 70 percent of its revenue comes from Medicare and Medicaid patients, these uncompensated costs can quickly take a toll.
The Root of the Problem: Urbanization and the Loss of Agricultural Jobs
However, the root of the rural hospital problem is much deeper than the failure of Medicare reimbursements to adequately fund hospitals. According to the Kentucky Center for Economic Policy, the total Kentucky population grew by 106,240 people between 2010 and 2017. This growth was not distributed evenly, though; the population in urban counties grew by nearly 4.7 percent, while the population in rural counties dropped by -0.7 percent. Despite the fact that the entire country has seen a trend of urbanization since the Great Recession, the expedited decline of coal and loss of manufacturing jobs in Kentucky is urbanizing the state at a faster rate than ever before, leaving rural areas with a shrinking population that tends to be older, poorer, and more likely to be uninsured or on Medicare or Medicaid.
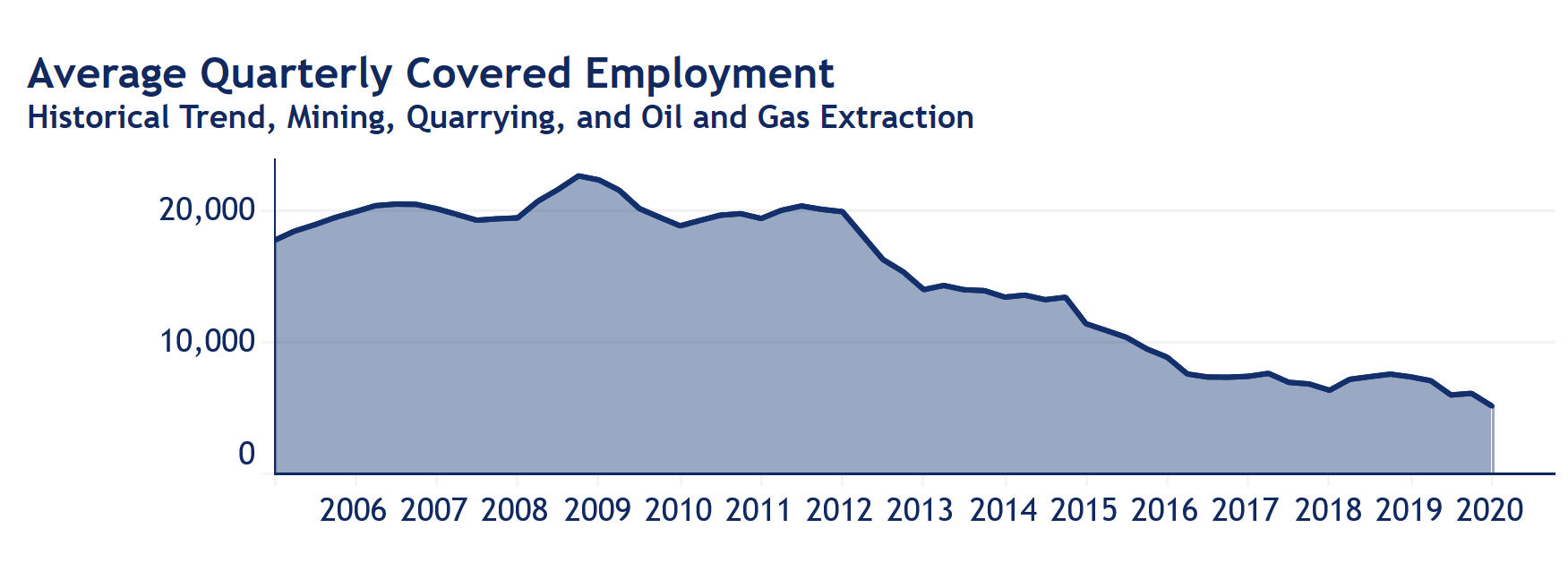
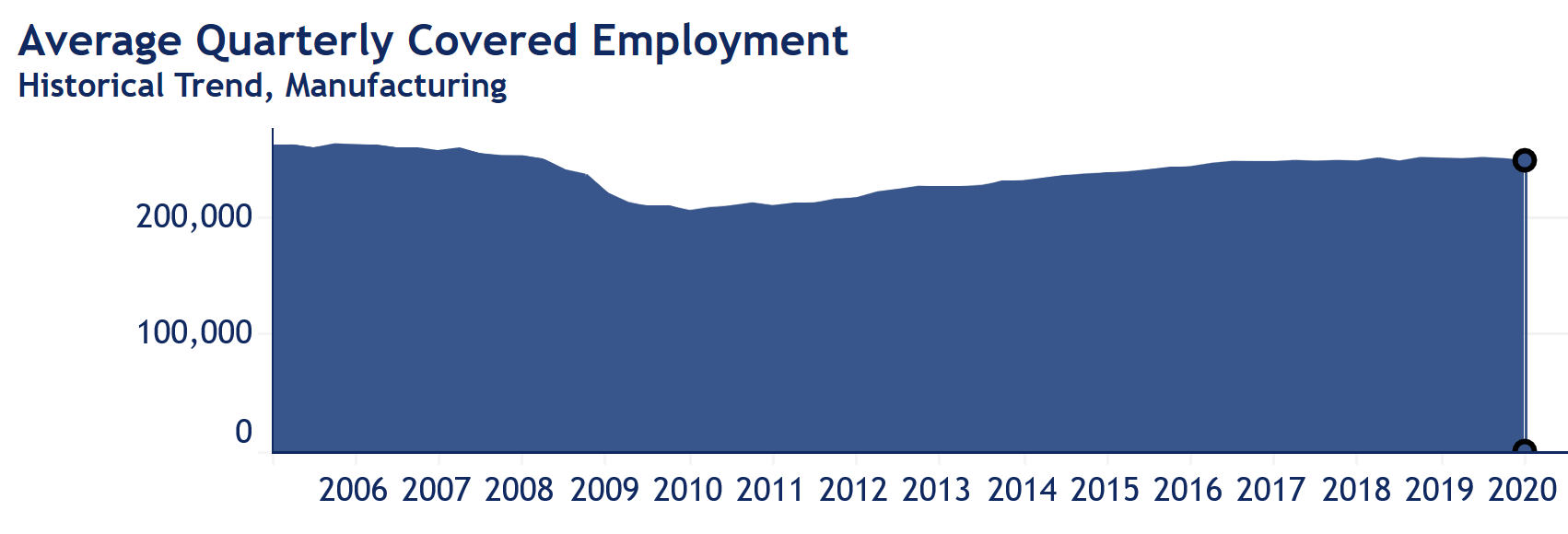
Source: KYStats Economic Activity Report
Preceding the recession in 2008, the mining and manufacturing industries employed nearly 283,000 Kentuckians or about one in five workers at the time. Since then, the mining industry has lost about 18,000 jobs and the manufacturing industry about 15,000. The relatively cheap prices of natural gas and environmental standards from the Obama Administration has most likely been the primary reason so many coal jobs have been taken away in Kentucky, as former power plant customers are now taking their business elsewhere and new regulations call for cutbacks in production. And likewise, the rise in technology has contributed to the loss of jobs in the manufacturing sector, as more manufacturing companies are beginning to rely less and less on actual workers and more on the technology which has replaced them.
Losses in both sectors can be attributed to the fact that more people are attending college and moving out of rural areas than ever before. Nearly 90 percent of millennials who graduated from high school attended college within eight years, where they went on to pursue jobs in medicine, law, and engineering in urban areas. And unfortunately, this is a trend that is not expected to change anytime soon; projections estimate that by 2050, nearly 87.4 percent of the U.S. population will be living in urban areas.
Ultimately, these trends have only exacerbated the failure of Medicare reimbursements to adequately fund rural hospitals, and thus, they are an important issue that needs to be addressed.
Making the Case for Rural Hospitals
When my hometown hospital went to the county fiscal court in 2018 proposing a 10 percent increase in countywide property taxes that would go back to the hospital, the community did not take it very well. In an agriculture-based county like mine, an increase in property taxes is essentially the last kind of proposal community members are willing to agree to. Opponents of the proposal argued that the hospital could be absorbed by a larger hospital in the near future, or, if all else fails, community members could easily travel to the next closest hospital for care in an emergency. Despite their arguments, many of those community members have benefitted from the welfare of the hospital without fully realizing it.
Like my county hospital, rural hospitals prove useful to their communities in a number of ways. For one, rural hospitals tend to be the locus of the health care systems in the community, directly employing and/or supporting many of the community’s health care personnel, such as those that work at the county clinic or the pharmacies it contracts with. Secondly, not only does the health sector constitute about 14% of total employment in Kentucky’s rural communities, but hospitals and the clinics they own are also one of the highest-paying employers in a rural area. Thus, a rural hospital closure has a significant economic impact on a rural community. A Health Services Research journal report found that when a rural area’s only hospital closes, per-capita income in that area drops by 4 percent, and the unemployment rate increases by 1.6 percentage points. This is a substantial effect considering most rural communities already face an increasing number of economic hardships.
The loss of rural hospitals also means that patients in those areas have to travel longer distances to the next medical provider, which could ultimately determine life or death for a patient. In most cases, the nearest hospital in a rural area can take anywhere between 35 minutes to an hour to travel to. A study conducted in 2015 found that rural residents that have to drive long distances to get primary care are less likely to seek recommended preventive services such as flu shots, blood pressure screenings, and cancer screenings. Because those that live in rural areas are already more likely to die from heart disease, cancer, unintentional injury, chronic lower respiratory disease, and stroke than their urban counterparts, lack of access to preventative care only perpetuates the rural health crisis. Thus, it is vital that steps be taken to improve the financial well-being of rural hospitals.
Big Problems Require Big Solutions
A problem as vast as the one confronting rural hospitals requires vast solutions. It is going to take more than simply cutting some operating costs and refinancing for rural hospitals to stay afloat, though this is often the first idea proposed to rural health care administrators. The easiest way for rural hospitals to become more prosperous and financially sustainable—while avoiding red tape— is to first seek new revenue sources.
One of the most common means to generate new revenue for a struggling rural hospital is to merge with a larger hospital system in the area. The premise behind this is that larger, urban hospital systems—like Baptist or KentuckyOne Health, for instance—absorb smaller, rural hospitals in order for the hospital to survive. In some cases, mergers with larger hospital systems can be incredibly beneficial to a rural hospital; this can potentially mean better physician recruitment, joint purchasing power, shared services, and most importantly, survival. However, many rural hospital administrators have expressed their concerns with the idea of a merger, as it has the potential to outsource support services, create an even longer commute for local residents seeking care, consolidate particular services that could reduce the number of local jobs, and take control and independence from the current hospital administration and personnel.
Another feasible solution for rural hospitals—and one that allows them to maintain their independence and services—is participation in the 340B Drug Pricing Program. This federal drug pricing program, created under the Public Service Health Act of 1992, provides considerable discounts on outpatient prescription drugs to hospitals, skilled nursing homes, pharmacies, and health care facilities by requiring pharmaceutical companies to charge less on prescription drugs for hospitals and clinics that serve high volumes of low-income patients. This allows eligible hospitals to buy drugs at a discount from the pharmaceutical companies, and then get reimbursed by Medicare for the full, non-discounted, price of the drugs. Thus, participation in this program gives rural hospitals an opportunity to make somewhat of a profit, which, in turn, they can use to cover some of their uncompensated care costs.
And lastly, the less likely, red-tape-entangled solutions are those that would have to come from federal and state governments. One hope is that Congress will permanently abolish Medicare sequestration efforts put in place back in 2013. These 2% budget cuts that have caused many rural hospitals to experience significant reductions in their reimbursements were originally scheduled to end in 2022, however, Congress recently reset them to expire in 2030. Rural hospitals need to be assured that these cuts are going to be removed indefinitely in order for hospitals to maintain any kind of long-term vitality. And on a state level, considering how the lack of skilled physicians in rural areas has affected how much money hospitals make, another potential solution would be for legislators to adopt incentives for providers who practice in rural, underserved parts of the state. Some states already offer financial incentives to encourage health professions students to pursue a career in primary care and practice in rural or underserved areas. These state programs are funded through different public and private sources. The National Health Service Corps State Loan Repayment Program, for example, provides cost-sharing grants to support 30 states to operate their own state loan repayment program. These incentives could attract a larger variety of doctors to the area and help close the gap between urban and rural health disparities while also improving the finances of many rural hospitals.
Although rural hospitals have long-faced exceptional circumstances that have hindered their health improvement efforts, it is becoming more and more apparent within recent years that these challenges are beginning to affect the vitality of the hospitals and, in turn, the economic health of their communities. Rural communities cannot afford to have economic and health conditions worsen any further, and thus, it is dire that hospital administrators, policymakers, and communities work together to find innovative solutions to solve the rural hospital problem in Kentucky.
Photo: Heather Boerner
